|
Special Report: Psychological MedicineA psychosomatic approachDAVID ZIGMOND, MB, ChB, MRCGP, DPM Psychotherapist, Department of Psychological Medicine, Hammersmith Hospital, London
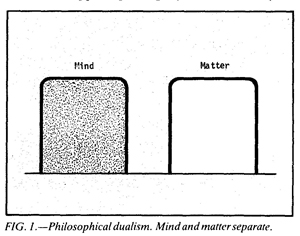
The very term 'psychosomatic' produces difficulties. It attempts to define patterns of physical distress or dysfunction which are not simply caused by physical determinants, and the structure of the word indicates an outlook in which mind and body are considered together. However, Western theory and practice of medicine is so thoroughly rooted in Newtonian scientific thought, a system which we rarely question, that the psychosomatic approach continues to evoke mystification, confusion and denial. The foregoing quotation perhaps encapsulates these reactions in a doctor adopting a defensive attitude to a psychosomatic viewpoint. This series of two articles explores and clarifies various aspects of the psychosomatic approach; they are not intended to be authoritative statements on the subject, the aim being rather to examine and speculate as to how different kinds of medical practice tackle this problem;, and how both patients and doctors perceive, and act upon, different parts of this problem at different times. The somatic approach To understand our difficulties with the psychosomatic* viewpoint, we need first to survey briefly the roots and assumptions of our present medical practice. Medicine and medical psychiatry are based on the disciplines of the (Newtonian) physical sciences and their underlying philosophies of dualism and determinism. Dualism, derived from the writing of Descartes, Malebranche and Geulinx (Russell, 1961) holds that the world is composed of two separate substances, matter and mind, which are independent but synchronous in activity; the two modes are governed by their own laws and run parallel courses (fig. 1).
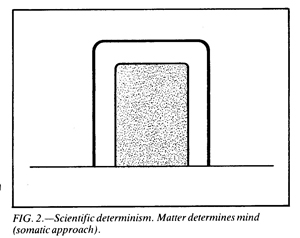
Newtonian physics and the consequent school of scientific determinism takes these assumptions ever further. There is an axiom here that only outwardly observable events (matter) are valid and `real'. Mind or experience are subsumed under the dictates and laws of this observable world in such a way that the subjective world ceases to be of importance, and is regarded as an artefact or interference. This scientific determinism is the root and prevalent philosophy in our present Western technological culture, where the bulk of our endeavours incline to engineering, that is, the direct alteration and control of physical structures. Medical practice, deriving from this outlook, is based on the assumption that distress can only be alleviated by changing behavioural or physical manifestations of that distress. Antacids for dyspepsia, tranquillizers for anxiety, and behaviour therapy for sexual dysfunction are clinical examples of this engineering philosophy. The experience of distress, it is held, will yield to control of its physical determinants; there is no need to explore or amplify the experience itself, as the experience is only a reflection of disturbed underlying mechanism.
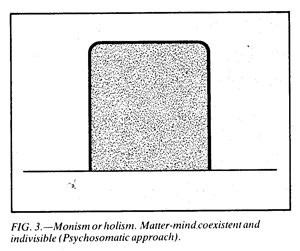
In clinical practice this approach may be termed `somatic', and an essential component of this system is the concept of physical causation (fig. 2). This defines events as being hierarchical in operation, so that one happening is rigidly determined by its material antecedent. Such a somatic-causational frame of reference is highly effective, even mandatory, in certain clinical situations; for example, when attending the patient with a perforated duodenal ulcer. At other times, however, it may be simplistic to the point of exclusion and distortion. An example of this might be the unhappy asthmatic child whose disease is said to be caused by house-dust mite allergy; even if the allergy is dealt with, he may still remain wheezy and, if the wheezing is controlled, he may well succumb to some other form of illness. Such problems are common in primary medical care, when simple physical diagnoses are evidently inadequate to explain the patient who suffers from a changing mosaic of apparently unrelated complaints, or the family which seems prone to perennial illness (Balint, 1957). Monism What is lacking in the latter situation is a holistic approach which deals with the person, his experiences and environment in a less piecemeal, and more global, manner. Philosophically this alternative approach has been termed monism and is represented in our culture by the philosophical writings of Spinoza and Bergson. Here there is no division of the world into mind and matter; there is only one substance which is experienced differently, internally as mind and externally as matter (fig. 3). The differences are due to the different positions of those undergoing the experiences, not the nature of events per se.
It is sometimes claimed that such an approach is unscientific but, in fact, it accords with the development of physics since Heisenberg (Russell, 1959) and Einstein (Einstein and Infeld, 1938). Relativity physics, for example, demonstrates that events and structures which appear to have a definite order or design to one observer, will show a different pattern to a differently placed observer. Consequently, the concept of causation breaks down, as one event does not necessarily precede another unless the frames of reference of the observers are similar. Physics overcomes this by fusing space and time which were previously conceived as inviolable and distinct. By analogy, a holistic approach integrates mind and body in the same way that relativity physics has fused space and time. Within this model it can be seen that there is not a simple causational (hierarchical) relationship between mind and body; they are merely different aspects of the organism. A change in the body is bound to be accompanied by a shift in mental equilibrium and vice versa. The two are co-existent and indivisible. While the deterministic approach looks for a causal relationship between mind and body, the holistic approach observes changes in the whole organism. An example of this can be illustrated by the two different views on an anxious person with ulcerative colitis. The somatic approach will conceive of the anxiety and colonic inflammation as being 'caused by' disturbances in neurotransmitters, inflammatory mediators etc. The psychosomatic approach will view the experience of anxiety and the signs of colitis as being manifestations of disturbance within the whole person and his environmental field; the inflamed colon and the experience of anxiety being the small part of the disturbance, which both patient and doctor are aware of at the present time. There are important theoretical and practical difficulties which arise from the traditional scientific method, and what can be contained within it. In the world of biology, science, as elsewhere, is confined to the outward and material manifestations of life. The inner experience, or mind, remains unobserved and thus outside strict scientific assessment of formulation. The nearest that such methods can get to the mind is through such signals as words and behaviour, from which we assume the inner experience. It follows that the somatic approach fits most comfortably within the scientific compass, while the psychosomatic method flows outside in many directions. The validity of the psychosomatic framework is, therefore, difficult to appraise objectively; as I shall suggest in the next article, it may only be practically effective if it has subjective meaning, particularly where the patient is concerned. This may account for the many confusingly inconclusive or negative studies which have been scientifically designed to discern components of 'anxiety' or 'depression' in illness, or the efficacy of psychotherapy in their relief. In these studies the immeasurable variables are subtle and possibly innumerable, so that studies of complex clinical problems necessarily reduce them to a somatic distillate; the psychological component having evaporated in the process. It is crucial to note that there is no 'right' or `wrong' approach. By analogy, relativity physics has not indiscriminately supplanted Newtonian physics. The two systems have different areas of operation and different yields. Sometimes the somatic approach is entirely satisfactory for the task at hand, at other times the psychosomatic approach will be more effective. Inappropriate use of the somatic approach leads to practice that is too simplified, unnecessarily intrusive or controlling, and alienating. On the other hand, when the psychosomatic approach is used indiscriminately it can lead to practice that is dangerously unfocused or inactive. It will be indicated later how there are often subtle factors of dependency, both in the patient and his doctor, which largely decide which kind of model is used in any particular medical situation. East and West At this point it is interesting to observe that different cultures have traditionally conceived the world differently, leading to contrasting types of medical practice. The West, which is increasingly influenced by a materialist-determinist philosophy and its consequent technology, has produced a pattern of medical practice which is strongly somatic in its bias; we consume an ever-increasing quantity of drugs to allay our discomfort or distress. Grief, despair, madness, or sexual disinclination, are all easily slotted into syndromes for which a prescription is found. The pursuit of the 'biochemical cause' of, for example, cancer and schizophrenia is to our technological culture what the Holy Grail was to early Christian societies. The results of such endeavours are often not dissimilar. Eastern and pre-industrial cultures are traditionally more monistic or psychosomatic in their approach; mind and body are not analytically dislocated as they are in the West. It is believed, therefore, that any attention to the body will change the mind, while calming the mind is bound to reduce disturbance in the body. The repertoire of resulting practices, which is extremely varied and often incomprehensible to those of us familiar only with Western practice, includes massage, yoga, incantation, exorcism, dietary rituals and acupuncture. At present many people are turning to these Eastern practices, which may reflect a disillusionment with the overgrowth of our medical technology and other cultural trends, experienced as controlling and depersonalising (Illich, 1976). Even the world of non-organic psychiatry is subject to this division. Traditional Western therapies evolved from a scientific-deterministic framework. Psychoanalysis, ultimately has its roots in Freud's training as a neurologist, and behaviour therapy is based on learning theory. In both the model of disturbance and therapy often incorporates the notion of a determining cause. Also, they tend to be applied within a highly defined mode of experience; the latter with overt behaviour patterns, the former with verbal communications. Some of the new humanistic therapies have attempted to incorporate Eastern monism. Gestalt (Perls et al, 1951) and bioenergetic therapy (Lowen, 1976), for example, regard bodily and mental experiences as being correlative and interchangeable. In these therapies there is equal attention paid to all forms of experience, sensation and behaviour. It is noteworthy, also, that the former types of therapy have found a place in the current realm of medical practice, while the latter have not yet found a comparable assimilation. The responsibility spectrum Illness, as usually conceived, is separate from the self as experienced in our conscious thoughts and feelings. It is something that 'happens to', or attacks, the self through organisms, accidents or fate. It is not usually considered as the expression or function of the self. The complex of intention, thought and feeling (the self) is thought to be quite different from the world of the body, much as a person and the house he lives in are thought to be distinct. This, of course, is the dualistic approach. The doctor's conception of illness, and its relationship to the self, often veers further towards the scientific-deterministic view, which sees a person as being controlled and defined by his body through genetics, chemical transmitters and the like. The quintessence of this approach is found in organic psychiatry, which considers mental and behavioural aspects of a person to be 'caused' by an underlying physical matrix. The fact that this matrix is often not well substantiated or defined does not detract from the influence of this model in practice (Zigmond, 1977). It can be seen that these two approaches see illness as 'ego-dystonic', that is, having no connection with conscious volition, feeling or responsibility of the self. Illness becomes a fault in the machinery of the body; such mechanisms being dictated by the impersonal forces of physics and chemistry. The person is merely a passive and powerless onlooker to his internal processes. Changing such processes, if possible, is seen as coming from the outside, through powerful agencies which manipulate the physical and chemical mechanisms. Alleviation of illness thus becomes the responsibility of the medical attendant, not the patient. When a person goes to a doctor as a patient he largely disowns and encapsulates his distressing experience, and expects the doctor to define it and take it away (Zigmond, 1977). Often, of course, this system is efficient and mandatory; a man with renal colic cannot be expected to make his own diagnosis and relieve his own pain. At other times, however, the issue is less clear-cut. Perhaps most primary medical consultations do not involve structural disease, but rather disturbances of function and bodily experience, which are related to conflicting and unexpressed feeling. Tension headaches, 'needing a tonic', nonspecific musculoskeletal and abdominal discomforts make up a large part, if not the bulk, of the primary doctor's work. Such complaints sometimes yield to suggestion and physical intervention alone. More often, however, this application of the Medical Model serves only to parry the distress syndrome for short periods of time. My next article will explore how application of other non-deterministic models may make more substantial therapeutic inroads into these clinical situations. If a person's distress is conceived by that person as an expression of inner conflict or turmoil, he is unlikely to think of himself as ill, merely distressed. In this instance the complaint is 'ego-syntonic' ; the bodily disturbance and the self are perceived as a unit. The sufferer sees his experience as being his responsibility; he may wish that someone (for instance a doctor) could assume responsibility for taking away his discomfort, but in reality he knows that this is not possible. If such a person asks for help it is for compassion, suggestions or new understanding, not magical exorcism. Naturally, it is uncommon for a person to contact his doctor from the outset with these notions, although he may acquire them through consultation. Such a process is called 'gaining insight', and marks a shift in the patient's thought and feeling process, from a dualistic/deterministic to a monistic/holistic approach to his distress. This change implies also a shift in ownership and responsibility of distress from the doctor back to the patient. It is an important intention of psychotherapy for psychosomatic complaints; in this area the aim of psychotherapy is to help the patient 'identify with' his symptoms so that they are seen as a reflection of feelings, needs or conflicts that are not being dealt with successfully in other ways. Such holistic awareness confers a creative meaning on symptoms; they become the body's signal of disequilibrium pushing into awareness, and providing the opportunity for exploration, expression or resolution. Understandably, many people are not able or willing to make this kind of reclamation as it involves feelings or conflict that are painful to acknowledge. Those who do so may only be able to make this transition with much support and guidance. How a person experiences, conceives and communicates physical distress and how the helper intervenes may be represented as in the table, below. Generally, traditional medical disciplines and skills operate best at positions (1) and (2) on the spectrum. Here the concept of illness is dealt with as an alien or malevolent intrusion into the self. Position (4) is juxtaposed to these in regarding illness as an expressive syndrome. Position (3) `it's just your nerves'is an interesting midway point; in return for the patient assuming partial responsibility for his dilemma, the doctor offers him a metaphorical structure upon which to hang this responsibility. A patient's 'nerves' imply an immutable and constitutional quality, and cannot be cured by the doctor as can an illness; nevertheless the patient may expect some kind of soothing or tranquillization of the metaphorical structure.
A clinical example Let us take a simple and common clinical example to illustrate some of the features of this spectrum. Mr A is a healthy young man who presents with cervical-occipital headaches for which no significant structural disease can be found. If he communicates his symptoms in wholly physical terms, and is accepted and dealt with at this level by the doctor, then both are functioning in position (1). The symptom is thought of as an excrescence; an autonomous disease focus to be cured or suppressed with drugs, while leaving Mr A himself immune from challenge or examination. The doctor calls Mr A's complaint 'fibrositis', and Mr A is pleased with this utterance as the mystifying nomenclature has taken his complaint away from him, and placed it in the province of medical science. The doctor has assumed responsibility for its definition and removal, and Mr A need not now worry about the meaning or nature of his bodily sensations. Suppose, now, that the doctor expands his questioning and elicits that Mr A feels worried, wakes early in the morning, is sexually disinterested and often feels like weeping, but does not yield to this. He cannot, or will not, disclose to the doctor why this should be so and the doctor does not pursue the meaning for the patient of this disturbed behaviour or experience, as he feels that he has reached his diagnosis of 'depressive illness with somatic manifestations' (position (2)). The phenomenon is now encapsulated into a framework that implies a physical causation for the distress, though less tangibly or specifically than in position (1). However, the doctor's tone and language convey authority and a technical understanding of the patient's experience, which both lie beyond the patient's sphere of influence. The doctor, in treating 'depressive illness', has assumed the bulk of the responsibility for the distress. The patient's expected role is to remain cooperative, that is, to do what the doctor suggests. Another doctor (or the same doctor on another day!) may not wish to assume this kind of responsibility. He may, too, be less convinced of the cogency of 'mental illness' as a workable diagnostic tool. He wants Mr A to assume responsibility for his plight, so he says 'Well Mr A, I've examined you and listened to your story and I'm quite sure that there's nothing seriously physically wrong with you to cause your headaches. I think we can put it down to your nerves. After all, you've always been a worrying type and you've also been under a lot of strain recently. Perhaps you need to take some time off work. These tablets might help, too, to relax your nerves'. There is an interesting shift in this consultation. At the beginning of the interview, doctor and patient conferred at position (1), but now the doctor has moved to position (3). He is willing to remain responsive to Mr A, but does not wish to assume total responsibility for his condition. If Mr A is responsive to this proposal, the consultation will move to a gratifying completion. Mr A will feel that he understands his complaint a little better, and the doctor may feel that he has shared his clinical responsibility rather more, thereby reducing his own burden. But Mr A may not be amenable to such a move. He may deny he is a worrier, though his friends and family clearly experience him as such. Or he may say (angrily) 'Yes, I am a worrier but that's got nothing to do with these headaches, they're terrible, you know'(!) Assuming the doctor has been tactful and competent, Mr A's communication to him now implies something like I don't wish to explore the nature or meaning of my discomfort, and I don't want to take any responsibility for it'. If the doctor does not respect this defence, and persists in operating from position (3), it is likely that he and the patient will swiftly reach an unworkable impasse. The situation is akin to the child who does not want to eat what is offered; the feeding adult may 'know' correctly or mistakenly that it is 'good for' the child, but until the child himself is willing to take it, all attempts at feeding will be met by various forms of sabotage. Overt refusal, hiding the food in the cheek or napkin, or vomiting it back, all have their analogues in the medical consultation and the more complex task of psychotherapy. In the above example it is likely that the doctor will retreat back to position (1), confirming his act with a prescription as a token of his (albeit ambivalent) medical responsibility. If Mr A responded readily to the doctor's suggestion of 'nerves', and showed an interest in how his complaint was associated with his feelings and relationships, the doctor may, if he has the time and interest, venture to position (4). If successful, Mr A will not be content merely to accept the label that he is a 'worrier' who suffers from 'bad nerves' but will want to integrate, understand and modify these mechanisms. He may see the doctor as a friend, a counsellor, a refuge in times of discomfort, but he does not expect technological magic or panaceas. In philosophical language he is perceiving himself `monistically' and his distress as an expression of himself, for which he, ultimately has responsibility. Naturally, such a position can seem frightening and lonely; it is often far more comforting to experience oneself dualistically, and have someone else take care of our distress and difficult feelings, while denying that there is a deeper or more extensive problem. It is interesting to observe how shifts in the spectrum may often work in the reverse way to these illustrations. In this case the patient will attempt to understand and integrate his illness holistically, while the doctor persists with a deterministic approach so that he can, without being undermined, assume his potent caretaking role (Zigmond, 1977, 1981, 1982). I remember a previously healthy man aged 80 years who developed lobar pneumonia soon after his wife died; I think I got this because of the wife going', he said to the doctor, 'I feel so lost I just don't want to carry on'. 'That's nothing to do with it', retorted the doctor authoritatively, but not unkindly, 'your pneumonia is caused by the pneumococcus germ'. True, the old man needed antibiotics, but perhaps his diagnosis was also correct, and could have been advantageously pursued. In such instances it is likely that it is the doctor, not the patient, who is unable to integrate certain kinds of feeling; perhaps this doctor was uncomfortable about his own feelings of grief or loss. In many medical consultations we are faced with this spectrum and options for changing our position. However, one of the rules of clinical communication is that consultation can only begin and go on with any viability if doctor and patient are operating from the same position and model. Likewise, there has to be accordance between patient and doctor for any shift to be beneficial; as the adage points out 'You can take a horse to the water, but you can't make him drink'. Reaching this common language and understanding is the central process in creating a therapeutic rapport. The route to such dialogue, as we have seen, is inevitably complicated by the distortions and resistances of both patient and doctor. Mr A represented what Michael Balint (Balint, 1957) termed 'unorganized (non-structural) illness'. My next article explores how these principles may be applied to organized (structural) illness. Figures (1), (2) and (3) are modified from Bertrand Russell's 'Wisdom of The West'. Rathhone 1959. Note *The terms 'psychosomatic' and 'somatic' are used in a particular way in this text which may not be in accordance with other writers. Some literature implies that psychosomatic illness is 'caused by' the mind and its conflicts. This article uses the word in a different sense, so that mind and body may be seen as equivalents and not necessarily as cause and effect. References Balint, M. (1957): 'The Doctor, His Patient and the Illness'. Pitman, London. Bergson. H. (1911): Creative Evolution. Macmillan. London. Einstein, A. and Infield, L. (1938): 'The Evolution of Physics'. Cambridge University Press, Cambridge. Illich, 1. (1976): 'Limits of Medicine, Medical Nemesis; The Expropriation of Health'. Penguin, London. Lowen, A. (1976): 'Bioenergetics'. Penguin, London. Perls, F., Hefferline, R., Goodman, P. (1951): Gestalt Therapy. Julian Press, New York. Russell,
B. (1977): 'An ABC of Relativity'. Allen & Unwin, London. Spinoza, B. de. (1955): Ethics. Dover, New York. Zigmond, D. (1977): Update, 15, 675. --------- (1977): Update, 15, 903. ----------(1981): Update, 23, 1811. ---------(1982): Update, 24, 281. This article first appeared in The Practitioner April 1982 Vol. 226. Contents Copyright ©; Dr David Zigmond 1982, 2010 Interested? Many articles exploring similar themes are available via David Zigmonds home page on www.marco-learningsystems.com David Zigmond would be pleased to receive your FEEDBACK
|